Critical Limb Ischemia
Critical limb ischemia (CLI)
What is critical limb ischemia?
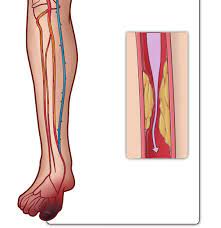
Critical limb ischemia (CLI) is a severe blockage in the arteries of the lower extremities, which markedly reduces blood-flow. It is a serious form of peripheral arterial disease, or PAD, but less common than claudication. PAD is caused by atherosclerosis, the hardening and narrowing of the arteries over time due to the buildup of fatty deposits called plaque.
CLI is a chronic condition that results in severe pain in the feet or toes, even while resting. Complications of poor circulation can include sores and wounds that won't heal in the legs and feet. Left untreated, the complications of CLI will result in amputation of the affected limb.
Symptoms of critical limb ischemia
The most prominent features of critical limb ischemia are called ischemic rest pain — severe pain in the legs and feet while a person is not moving, or non-healing sores on the feet or legs. Other symptoms include:
- Pain or numbness in the feet
- Shiny, smooth, dry skin of the legs or feet
- Thickening of the toenails
- Absent or diminished pulse in the legs or feet
- Open sores, skin infections or ulcers that will not heal
- Dry gangrene (dry, black skin) of the legs or feet
Risk factors of critical limb ischemia
Risk factors for chronic limb ischemia are the same as those for atherosclerosis -- hardening and narrowing of the arteries due to the build up of fatty deposits, called plaque. The following all contribute to this condition:
- Age
- Smoking
- Diabetes
- Overweight or obesity
- Sedentary lifestyle
- High cholesterol
- High blood pressure
- Family history of atherosclerosis or claudication
Treatment for critical limb ischemia
Critical limb ischemia is a serious condition that requires immediate treatment to re-establish blood-flow to the affected area. The number one priority is to preserve the limb.
Endovascular treatments
Minimally invasive endovascular therapy is often an option in the care of CLI. The treatment recommended depends on the location and severity of the blockages. Most patients with CLI have multiple arterial blockages, including blockages of the arteries below the knee. In general, puncture of the groin, under local anesthesia, with insertion of a catheter into the artery in the groin will allow access to the diseased portion of the artery. Some of the endovascular procedures used to treat CLI include:
- Angioplasty: A tiny balloon is inserted through a puncture in the groin. The balloon is inflated one or more times, using a saline solution, to open the artery.
- Stents: Metal mesh tubes that provide scaffolding are left in place after an artery has been opened using a balloon angioplasty.
- Laser atherectomy: Small bits of plaque are vaporized by the tip of a laser probe.
- Directional atherectomy: A catheter with a rotating cutting blade is use to physically remove plaque from the artery, opening the flow channel.
Recovery from these procedures usually takes one or two days.
Surgical treatments
Treatment of wounds or ulcers may require additional surgical procedures or other follow-up care. If the arterial blockages are not favorable for endovascular therapy, surgical treatment is often recommended. This typically involves bypass around the diseased segment with either a vein from the patient or a synthetic graft. Hospitalization after a bypass operation varies from a few days to more than a week. Recovery from surgery may take several weeks.